By the Calorie Control Editorial Team
The etiology of type 1 and type 2 diabetes differ, but they share similar goals for medical nutrition therapy to help manage the disease and reduce potential complications from poor glycemic, lipid and blood pressure control. Evidence-based nutrition practice guidelines are essential for health professionals to provide the best interventions to reach these goals. These guidelines are based on recommendations developed by diabetes experts who periodically review the scientific literature for new studies on dietary factors affecting diabetes, and then grade the strength of each study to weigh their impact on clinical application. Recommendations regarding the use of nonnutritive sweeteners (NNS), like aspartame, from three professional associations are provided below.
American Diabetes Association (ADA) “Nutrition Therapy Recommendations for the Management of Adults with Diabetes” (2013 ).
“Use of NNSs has the potential to reduce overall calorie and carbohydrate intake if substituted for caloric sweeteners without compensation by intake of additional calories from other food sources.”
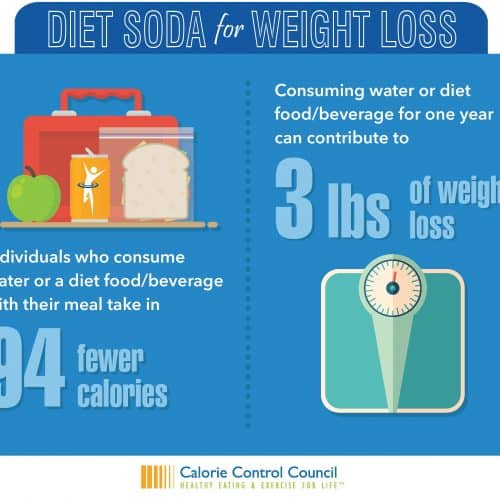
A study by Tate et al., provides another potential benefit of NNS for individuals with diabetes that supports the objectives of the ADA. When caloric beverages were replaced with noncaloric beverages or water for the purposes of weight loss in the CHOICE Trial they found those in the Diet Beverage group (containing NNS) had a greater reduction in caloric intake that those in the Water group. The authors concluded the use of diet beverages may support greater adherence to prescribed dietary patterns by improving palatability and enjoyment of foods and beverages.
American Dietetic Association (renamed the Academy of Nutrition and Dietetics in 2012) “Evidence for medical nutrition therapy for type 1 and type 2 diabetes in adults” by Franz et al. (2008).
“If persons with diabetes choose to consume products containing FDA-approved NNS at levels that do not exceed the ADIs (Acceptable Daily Intakes), the RD should advise that some of these products might contain energy and carbohydrate from other sources that needs to be accounted for. However, research reports NNS intake does not effect changes in glycemic response.”
American Heart Association (AHA) and American Diabetes Association Joint Scientific Statement on “Nonnutritive Sweeteners: Current Use and Health Perspectives” by Gardner et al. (2012).
“The evidence reviewed suggests that when used judiciously, NNS could facilitate reductions in added sugars intake, thereby resulting in decreased total energy and weight loss/weight control, and promoting beneficial effects on related metabolic parameters. However, these potential benefits will not be fully realized if there is a compensatory increase in energy intake from other sources.”
In addition to the research behind these clinical practice guidelines, several other reviews have been conducted to evaluate the effect of NNS on blood glucose management in recognition of the fact that individuals with diabetes are likely consume more NNS than non-diabetics. Studies involving aspartame and individuals with diabetes have been conducted since its inception and submitted as part of its initial approval process and ongoing surveillance. These studies were reviewed by Butchko et al., in 2002, who reported no adverse effects from aspartame were observed in subjects with diabetes. Subsequent studies reviewed by Magnuson et al., in 2007 also concluded aspartame ingestion by diabetic and non-diabetic individuals has no effect on blood glucose homeostasis.
“Overall, the vast majority of studies do not show any acute effects of IS [intense sweetener] intake on blood glucose or insulin concentrations measured on an empty stomach or after a test meal, in healthy subjects or in diabetics. Some studies reported a modest increase in GLP-1 [Glucagon-like peptide-1] secretion*, but with no repercussions on insulin secretion or blood glucose concentrations. IS consumption has no effect on short- and medium-term blood glucose parameters in healthy subjects or in diabetics.”
* GLP-1, a gastrointestinal hormone that usually increases insulin secretion, slows down gastric emptying and reduces glucagon secretion
Research claiming an association between NNS and diabetes must be evaluated against this existing body of evidence. There is no justification for a change in nutrition practice guidelines regarding the use of NNS by individuals with diabetes based on observational studies since they do not prove causality and have been unable to rule out confounding factors, as reported by Romo-Romo et al., (2016). Their review of the effects of NNS on metabolic diseases, including its effect on glucose metabolism, found the studies that claimed an association between the ingestion of low-calorie sweeteners and type 2 diabetes were unable to rule out increased body mass index, family history of diabetes and other changes in health status as confounding factors. Additionally, many of the studies didn’t distinguish among the different low-calorie sweeteners consumed, only evaluated “diet soda” intake and not table-top sweeteners and foods made with low-calorie sweeteners, and failed to track when the use of NNS was started relative to other dieting behavior or changes in body weight. They also found results of some of the clinical trials showing effects of NNS on glucose metabolism were contradictory due to confounding variables not mentioned or adjusted for in the studies.
In their discussion, Romo-Romo et al., state well-controlled randomized clinical trials in humans are not available to explain mechanisms that might cause changes in glucose metabolism after long-term exposure to individual NNS. Based on the evidence reviewed, however, they conclude that NNS can be considered a useful tool in the nutritional treatment of certain metabolic diseases, including diabetes, as a sugar substitute as long as the amounts consumed are within the ADI without caloric compensation from other foods.
People with diabetes seeking information about low-calorie sweeteners can view the What Can I Eat and What Can I Drink pages provided by the ADA for further guidance.